Treatment Options for Dental Unit Waterlines

Maintaining safe and compliant dental unit waterlines (DUWLs) is not just a box to check. It is a core part of infection control, patient safety, and practice readiness for audits or inspections. Because DUWLs use small diameter tubing and experience frequent stagnation, biofilm can develop quickly and persist quietly. The result is often a gap between what the water looks like and what the test result says.
Most practices set their water quality goal around the benchmark referenced by the Centers for Disease Control and Prevention (CDC) and the American Dental Association (ADA): dental treatment water for nonsurgical procedures should be at or below 500 CFU/mL of heterotrophic water bacteria (aligned with the Environmental Protection Agency drinking water standard). Reaching that goal consistently requires two fundamentals: using an appropriate water treatment modality and verifying its performance with routine testing.
A practical guide for dental teams who want compliant water without guessing.
Jump to:
Option 2: Straws and Cartridges
Option 3: Shock Protocols Only
Option 4: Water Treatment Systems
What the Target is and Where it Comes From
CFU stands for colony forming units, a way to estimate the number of viable bacteria present in water. The 500 CFU/mL threshold is widely used because it aligns with drinking water expectations and provides a clear, measurable benchmark for dental treatment water. For dental teams, this number becomes a practical decision point. If results are consistently at or below the threshold, your protocol is working. If results rise above it, you need remediation and a plan to prevent repeat failures.
This guide reviews four common approaches to DUWL treatment and explains how to choose a protocol that your team can execute and verify.
These categories are intentionally brand neutral. Always follow your dental unit manufacturer guidance and the treatment product instructions for use, including any compatibility notes and required monitoring.
Four Primary Treatment Categories:
Daily tablets added to self-contained bottles
Straws and cartridges installed in bottles or direct feed systems
Shock protocols only (periodic high-level disinfection without continuous treatment)
System produced water approaches (source water and fully treated water)
Each treatment approach above can be successful when built out with the correct full picture protocol. And each treatment approach can have gaps if not implemented properly. This blog article will explain the various options, benefits, and considerations and how to implement them into comprehensive protocols that build the right foundation for success.
Start With the System You Have
(and a baseline result)
Before comparing treatment options, map your actual water pathway. Are you running self-contained bottles in each operatory, a centralized bottle that feeds multiple chairs, or municipal/direct-feed water that enters each unit through plumbing? Do you have any inline filtration, softening, or other building-level water chemistry factors that could affect performance?
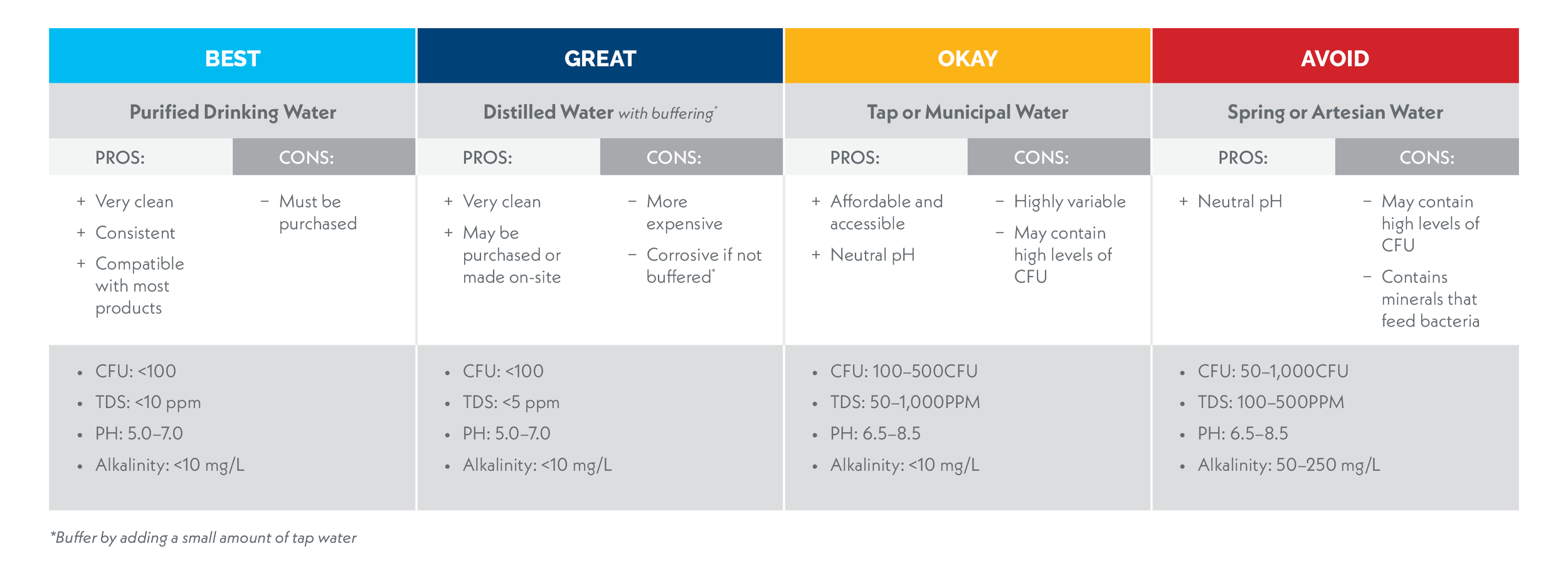
After determining how the water is delivered to your chairs, establish what kind of water you are or will be using. The type of source water used may have a direct impact on which treatment methods will be most effective. For a detailed explanation of common source water types used, see our blog Source Water Options: Selecting the Right Water for Your Dental Practice.
Next, decide who owns the process. The biggest failures in waterline safety are rarely about “bad products”—they’re about inconsistent execution: missed bottle changes, skipped shock cycles, undocumented deviations, or a protocol that lives in someone’s head instead of in writing. Assign a primary and a backup owner, write the steps into a waterline management Standard Operation Procedure (SOP), and make it easy to verify completion (checklists, logs, and reminders).
Finally, get a baseline waterline test result. A baseline establishes whether you’re starting with already low bacteria counts that just need maintenance or elevated counts and mature biofilm that require remediation first. It also gives you a reference point when you change anything (treatment type, source water, new chairs, long closures, plumbing work, etc.). StandardCheck includes photo documentation of the cultured bacteria, which can be a great baseline test to use for educating your office on what can be lurking within waterlines. RapidCheck not only provides results in 24 hours but also captures the widest range of bacteria in water samples, making it a great baseline test option as well.
Option 1: Daily Tablets

Daily tablets are a common choice for practices using self-contained bottles because they align with a routine task the team is already doing: refilling bottles. In general, these products are designed to release a low-level antimicrobial agent into the bottle water so that, once it reaches the waterlines, it suppresses microbial growth and helps maintain counts below target limits.
The key word here is maintain. Continuous, low-level treatment can be very effective when your lines are already under control. But if you’re starting with high counts, odor, or a history of failed tests, daily tablets alone may not be enough to penetrate established biofilm. In those cases, practices often need an initial remediation step, commonly a shock procedure, before a daily maintenance product can reliably keep you compliant.
Why Teams Like Tablets
Workflow Fit: integrates into bottle refills with minimal additional equipment
Scalability: straightforward to standardize across multiple operatories
Versatility: effective in the widest range of source water types
Consistency: provides the same dose of antimicrobial agent so long as IFUs are followed
Continuously Present: provides ongoing, constant treatment
Affordable: frequently on the lower end of treatment costs
Common Tradeoffs to Plan For
Human-factor Dependence: Missed doses (or inconsistent bottle volume) can translate to performance gaps.
Startup Sensitivity: If biofilm load is high, tablets may be ineffective against ongoing bacteria and biofilm growth until remediation is performed.
Compatibility and Chemistry: Daily tablets are not a universal fit - their performance can vary based on source water, bottle size, and dosing accuracy. Product instructions should be followed closely.
By-Products: Tablet ingredients may bind with minerals in the source water, creating solid precipitates that can discolor the water and bottle over time.
Execution Tips that Improve Reliability
Standardize the refill routine. Use the same bottle and fill volume each time and train to that standard. Decide on a single, reliable water source and always use the same one.
Build a “no-skip” cue. Store tablets in the same place so the step can’t be forgotten.
Consider a presence indicator. Some tablets have food safe dyes built in to tint the water so you always know if the antimicrobial is present. Another option is placing a tag around the neck of the bottle to indicate treatment is in use.
Document bottle changes. A simple log (date/initials/operatory) makes gaps visible.
Keep water flowing. Stagnant water is one of the leading culprits of waterline failures. If a chair or specific lines don’t see frequent use, be sure to regularly flush these lines to always keep fresh antimicrobial present.
Plan for closures. Long weekends and vacations change stagnation time; align your protocol with manufacturer guidance for idle periods.
Verify with testing. Early in a new protocol, test more frequently until you see stable passing results, then adjust to quarterly testing.
For any continuous tablet program, verification testing should be routine and documented. When you first implement tablets (or after remediation), consider testing sooner rather than later to confirm the protocol is working in your specific equipment and water conditions. After you establish consistent performance, maintain a regular cadence based on manufacturer recommendations, risk tolerance, and any applicable state or organizational requirements.
Option 2: Straws and Cartridges
“Straws” (for self contained bottles) and inline cartridges (for direct feed systems) aim to reduce day to day variability by making treatment more automated than manual. Instead of asking the team to add a tablet with every refill, these devices treat water as it passes through the bottle or supply line, providing continuous antimicrobial activity when used as directed.In a bottle based setup, the straw sits inside the bottle and treats the water in the reservoir as it passes through to the handpieces.
In a direct feed configuration, an inline cartridge is installed upstream of the dental unit. Each design has its own replacement intervals, water chemistry assumptions, and compatibility notes. The operational “win” is only real if your team replaces components on schedule and follows both the device instructions and your equipment manufacturer’s guidance.
Why Teams Like Installed Treatment
Reduced daily variability: fewer steps at each refill can mean fewer missed opportunities.
Clear replacement cadence: many practices find it easier to manage “replace on date” than “dose every time.”
Good fit for multi-chair consistency, especially in DSOs or practices with rotating assistants.
Common Tradeoffs to Plan For
Replacement discipline is essential: letting an installed device run past its effective life can look like “treatment is in place” while performance silently degrades.
Shock events still matter: continuous treatment is often most effective when biofilm load is controlled. Many protocols still incorporate periodic shock/remediation, especially after failures, long closures, or equipment changes.
Process complexity during remediation: depending on the system, you may need a temporary bypass/dummy component during shocking to protect or remove the installed device. Plan this ahead so remediation doesn’t stall.
Implementation Tips
Use a single “replacement day” policy. A monthly or quarterly standard date reduces missed intervals across operatories.
Track by operatory, not by memory. Label bottles or units and log installation dates where everyone can see them.
Align with your water source. If you switch source water (distilled vs municipal vs treated), treat it like a process change and verify performance.
Keep remediation supplies on hand. If a test fails, delays often happen because the practice doesn’t have what it needs to shock and retest promptly.
Verify replacement requirements. Some products require replacement after a certain number of days, liters of water, or if the antimicrobial released falls below a certain threshold (iodine or silver levels).
As with tablets, installed treatment should be validated with routine water testing. The most useful test strategy is one that includes (1) confirmation testing after initial installation or any major change, (2) routine monitoring on a set cadence, and (3) follow-up testing after any remediation event. This creates a closed loop where decisions are based on data, not assumptions.
Option 3: Shock Protocols Only

Some practices ask a direct question: “What if we just shock the lines on a schedule and skip daily tablets or straws?” The honest answer is that a shock only approach can work as a treatment, but it is also the option most likely to drift out of compliance without anyone noticing unless you test very frequently. For this reason, it is not generally recommended.
Here’s why: shocking is an event, not a continuous control. A high-level disinfectant may significantly reduce planktonic bacteria and disrupt biofilm, but DUWLs are engineered in a way that favors regrowth—especially with intermittent use, warm ambient temperatures, and periods of stagnation. Without an ongoing maintenance product, bacterial counts can rebound between shock cycles. That rebound may be slow and subtle, or it may be fast depending on your starting biofilm load, water chemistry, unit design, and day-to-day usage patterns.
Additionally, shock products are often more aggressive on dental equipment. Because this approach requires more frequent shocking, dental equipment may wear more quickly.
If you choose a shock only approach, frequent verification testing should be built into the protocol as a regular step, not an occasional audit. Testing is the only way to confirm that water quality remains at or below your target between shock events. A practical approach is to test soon after a shock to confirm effectiveness, then test again within a shorter interval to determine how quickly, or whether, counts rebound in your environment. If results trend upward or exceed your action level, the protocol needs to change. You may need to shorten the shock interval, test interval, improve execution, or add a continuous maintenance method.
When Shock-only Is Most Commonly Considered
Short-term remediation bridge: while waiting to implement a continuous program (tablets, straws, cartridges) or while troubleshooting repeated failures.
Very low use operatories: where daily dosing is frequently missed due to infrequent refills (though stagnation risk may increase). Mobile dentistry may be a good fit for shock only processes.
Operational constraints: where leadership is prioritizing the simplest possible workflow, recognizing that simplicity must be offset by more frequent testing and documentation.
Because shock chemistries, contact times, and flushing requirements vary widely by equipment and product instructions, the safest approach is to follow your dental unit manufacturer’s guidance and the shock product’s instructions for use. What matters most from a risk-management perspective is not the label on the bottle; it’s whether your process is executed correctly, documented, and verified with data.
Shock-only: A Minimum Framework For Safer Use
Define an action level and response plan. Decide in advance what result triggers immediate re-shock, intensified monitoring, or escalation.
Verify shock effectiveness. Test after shocking to confirm you achieved the expected reduction.
Measure rebound. Test again at a defined interval to learn how quickly counts rise without continuous treatment.
Document every event. Date/time, operator, units treated, deviations, and test results should be recorded.
Escalate quickly after failures. Repeated failures are a signal that biofilm control is not being maintained, and the protocol needs to change.
Testing Expectations For Shock-only Protocols
When shock is your only primary control, testing becomes the tool that keeps you honest. Plan to test after each shock to confirm the procedure worked, and test again between shocks to evaluate rebound. In many practices, this means testing more often than you would under a well-controlled continuous maintenance program, especially during the first months while you are learning how your waterlines respond.
Option 4: Water Treatment Systems
A fourth category to consider is treated water itself: not just what you add to the bottle, but the type of water you start with and whether that water is simply purified or actively treated for microbial control. This matters because practices often group these systems together even though they do different things. Some approaches focus on improving source water quality. Others are designed to help control bacteria within the dental water environment.
In general terms, reverse osmosis (RO) water is filtered to reduce many dissolved contaminants and is often used as a cleaner source water for dental bottles or delivery systems. Deionized water (DI) takes it a step further and removes charged minerals but does not, by itself, function as a continuous antimicrobial treatment for dental unit waterlines. Fully treated water systems go even further by pairing purification with an antimicrobial treatment strategy intended to help control bacterial growth in the water pathway. The key distinction is simple: RO and DI improve the quality of the incoming water, while fully treated water systems add a residual antimicrobial such as silver to eliminate the need for additional treatment—like building the tablet or straw directly into the system.
For practices using tablets or straws, starting with RO/DI water is often a good practice because it gives the maintenance product a more consistent source of water to work with. As always, the right choice depends on your equipment layout, manufacturer guidance, and protocols.
How These Approaches Differ In Practice
RO/DI water: a strong source-water option when the goal is cleaner input water and more consistent performance from tablets, straws, or other maintenance products.
Fully treated water: combines purification with an antimicrobial strategy intended to actively support bacterial control within the system and chairs. Look for systems that impart an antimicrobial such as silver or iodine into the water.
System choice matters most when paired with a written protocol, replacement schedule, and routine verification testing.
Because system designs, treatment mechanisms, and maintenance requirements vary, the safest approach is to match your source water and treatment method to your unit manufacturer guidance and your team’s actual workflow. What matters most is whether the approach supports ongoing bacterial control in your specific setup and whether testing confirms that performance over time.
Best Practices For Water Treatment Systems
Define the water source clearly. Know whether each unit is using municipal, distilled, RO, DI, or fully treated water.
Do not assume purification equals bacterial control. Clarify whether your approach is source-water improvement only or also includes active antimicrobial treatment.
Pair source-water decisions with the right maintenance method. RO water is often a strong companion to tablets or straws when those products are part of the protocol.
Document change intervals and maintenance steps. Filters, cartridges, bottles, and treatment components should be tracked by date and operatory.
Verify with testing. Any system claim should ultimately be confirmed by routine water quality results.
Testing Expectations For System-based Approaches
When you change source water, install a treatment system, or move from standard bottle water to a more advanced treated-water approach, testing should follow the change. Confirm performance after implementation, then continue a routine cadence to make sure the system is doing what you expect. This is especially important when teams assume that “purified” automatically means “compliant.” In dental unit waterlines, compliance comes from verified microbial performance, not from labels alone.
Conclusion
There is no single “best” dental water treatment option for every practice. The best option is the one that fits your equipment, your workflow, and your team’s ability to carry it out consistently. Tablets, straws, shock protocols, and water treatment systems can all play a role when they are used correctly and supported by routine testing. The common thread across every successful program is not the label on the product. It is a written process, clear accountability, and verification that your water is staying at or below the accepted benchmark. In other words, if you want confident compliance, choose a system your team can actually maintain and prove. And if you want a simple way to verify that your program is working, Agenics water testing can help you monitor performance, document results, and stay ahead of issues before they become failures.
-
American Dental Association. (2024, May 31). Dental unit waterlines. https://www.ada.org/resources/ada-library/oral-health-topics/dental-unit-waterlines
Centers for Disease Control and Prevention. (2024, May 15). Best practices for dental unit water quality. https://www.cdc.gov/dental-infection-control/hcp/dental-ipc-faqs/best-practices-dental-unit-water-quality.html
Agenics Labs. (2025, November 24). Dental water sampling best practices. https://www.agenics.net/blog/2025/11/24/sampling-best-practices
Agenics Labs. (2025, November 17). Dental waterline shocking: Best practices for safe & effective biofilm removal. https://www.agenics.net/blog/2025/9/23/shocking-best-practices